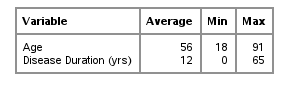
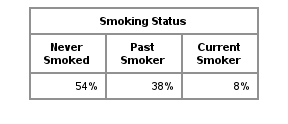
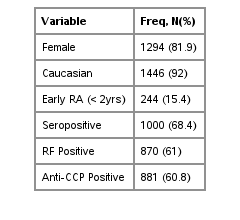
Characteristics of BRASS Subjects at Time of Enrollment1581 Patients Enrolled as of April 2025
Definitions:
RF Positive: Rheumatoid factor (RF) is a blood test that measures the amount of the RF antibody in the blood. It is one of the tests that physicians use to help diagnose RA. An abnormal result means the test is positive, which means higher levels of rheumatoid factor have been detected in your blood. In BRASS, a RF level of greater than 15 IU/mL is considered positive.
Anti-CCP Positive: This blood test detects antibodies to cyclic citrullinated peptide (anti-CCP) and is another blood test used to help diagnose RA. An abnormal result means the test is positive, which means higher levels of Anti-CCP have been detected in your blood. In BRASS, an Anti-CCP level of greater than or equal to 20 U/mL is considered positive.
Seropositive: If either of the RF test or Anti-CCP test is positive, a patient is considered seropositive. Seropositive patients have a greater likelihood of developing more serious disease. They are also more likely to have extra-articular complications (such as nodules and vasculitis) than those who are seronegative.
Disease Activity
Measures of Disease Activity Over Time
Click on graph for larger image
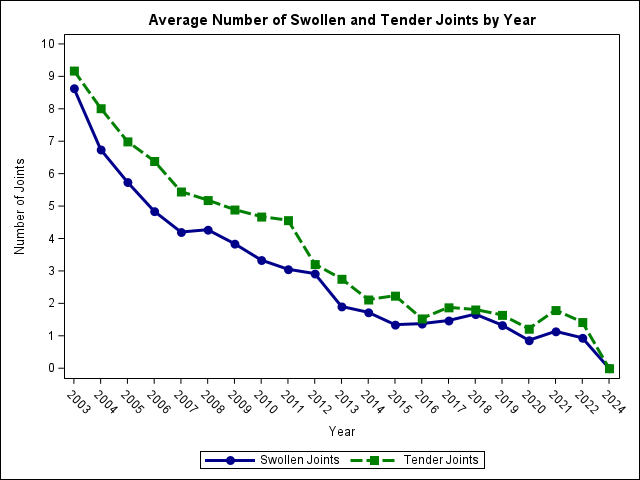
Joint Count
Swollen and tender joints are the most common symptoms of RA, and disease severity is directly related to the number of swollen and tender joints. There are many different methods for counting the number of joints involved in RA. The 28-joint count is used in BRASS. It includes shoulders, elbows, wrists, MCPs, PIPs, and knees, but excludes joints of the feet. This exclusion is because feet abnormalities may often result from things other than arthritis and for our research about RA, it would be difficult to separate out the non-RA effects on the feet. The exclusion of these joints does not discount their importance in routine clinical care because they may be a major source of discomfort and disability.
When looking at the graph, you’ll notice a sharp decrease in the average number of swollen and tender joints over the years. One explanation might be the introduction of biologic DMARDs (example: Enbrel, Rituxan, Orencia, Actemra). The first biologic DMARD was approved by the FDA in 1998, and following that, many new biologic DMARDs have been introduced onto the market over the years.
Click on graph for larger image
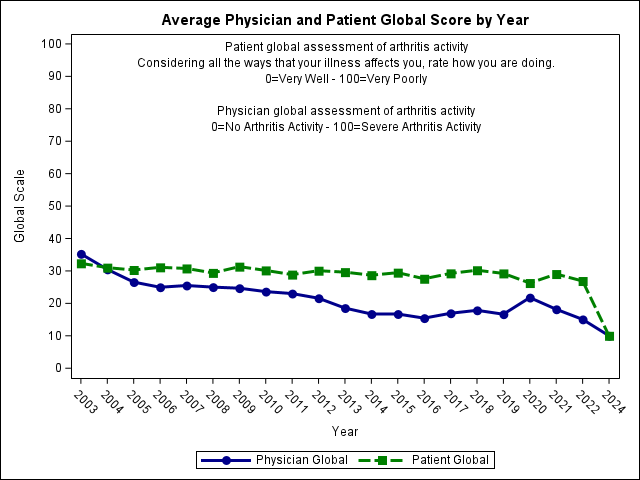
Patient Global
The patient global assessment of disease activity is a simple way of measuring the overall way RA affects a patient at a point in time. In BRASS, it asks, “Considering all of the ways that your illness affects you, rate how you are doing?” The best (lowest score) of 0 is labeled “Very Well” and the worst (highest score) of 100 is labeled “Very Poorly” with increments of 5 in-between.
Physician Global
Just like the patient global assessment, the physician global assessment is a way of measuring the overall way RA affects a patient at a point in time. It generally includes a statement such as “What is your assessment of the patient’s current disease activity?” The best (lowest score) of 0 is labeled “No Arthritis Activity” and the worst (highest score) of 10 is labeled “Severe Arthritis Activity” with increments of 1 in-between. In the graph above, it has been transformed to be on a 0 to 100 scale to match the patient global assessment.
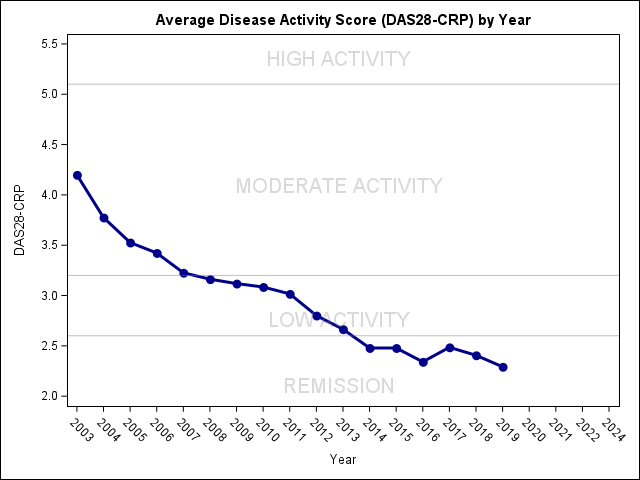
Click on graph for larger imageDAS28-CRP
The DAS28-CRP is a measure of disease activity in RA. Originally it was developed by Dutch rheumatologists for the purpose of comparing results in clinical trials of new drugs for treating RA. It has since become widely used as an outcome in various types of research concerning RA. DAS stands for ‘disease activity score’, the number 28 refers to the 28 joints that are examined for this assessment, and the CRP indicates a C-reactive protein blood test is used.
The DAS28-CRP score is calculated by using 4 measures of disease activity.
The number of swollen joints (out of the 28)
The number of tender joints (out of the 28)
The CRP blood test – a blood test looking for markers of inflammation
The patient’s ‘global assessment of health’ (a range between 0 and 100 where 0 is very good health and 100 is very bad health)
These results are fed into a mathematical formula to produce the overall score. The score can be broken-up into different categories of disease activity.
>
5.1 High disease activity
3.2 – 5.1 Moderate disease activity
2.6 – 3.2 Low disease activity
< 2.6 Remission of disease
Physical Function and Pain
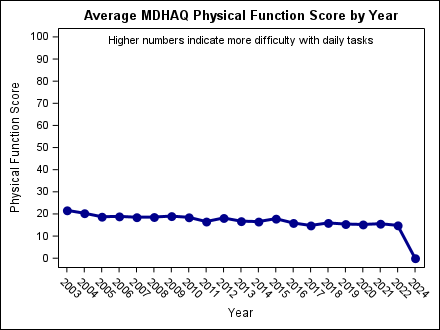
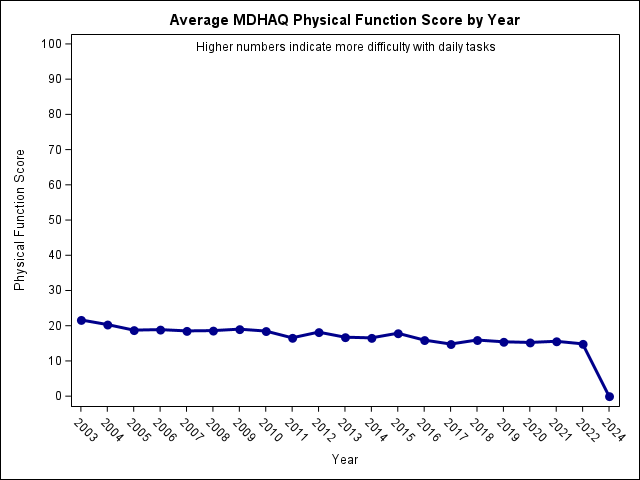
MDHAQ Physical Function Score The multi-dimensional health assessment questionnaire (MDHAQ) was designed to obtain patient-reported outcomes on different aspects of how RA affects their daily life. A physical function score is determined by asking 10 questions about their ability to perform daily tasks such as walking 2 miles, buttoning a shirt, and turning on a faucet. There are 4 choices for each question, “without any difficulty”, “with some difficulty”, “with much difficulty”, and “unable to do.” A final score is calculated and, in BRASS, transformed to be on a 0-100 scale. A higher number indicates more difficulty with performing daily tasks.
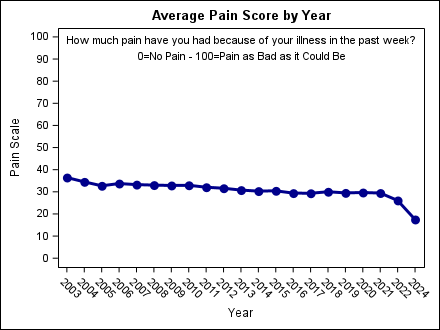
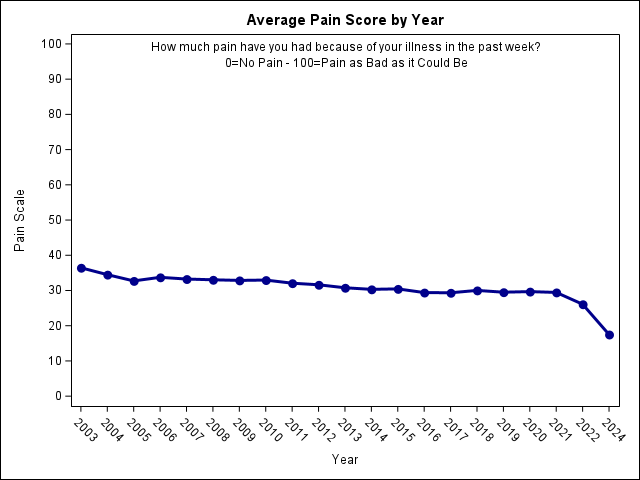
Pain ScoreThe pain question is a measure of pain intensity, which has been widely used in diverse adult populations, including those with rheumatic disease. In BRASS, the question is as follows:
Sleep/Fatigue
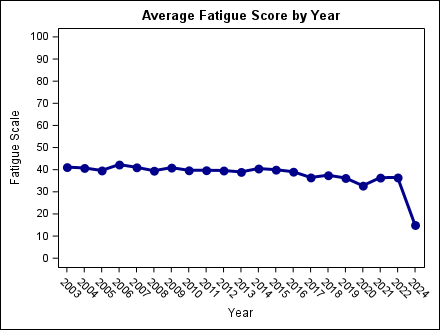
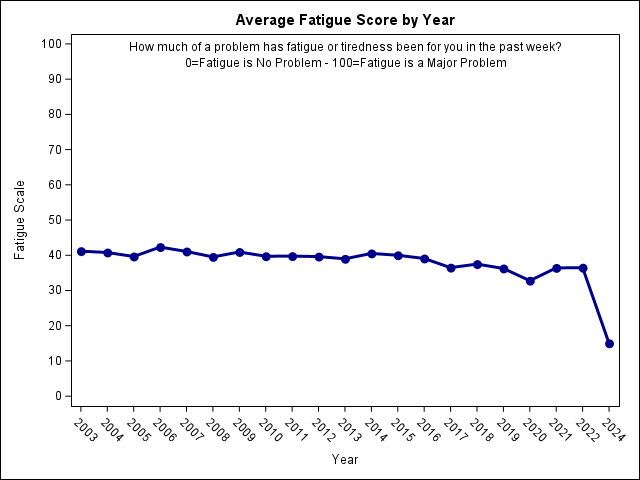
Fatigue ScoreFatigue is common to all the rheumatic conditions in varying degrees. The fatigue score is calculated from one question, with higher numbers indicating more fatigue.
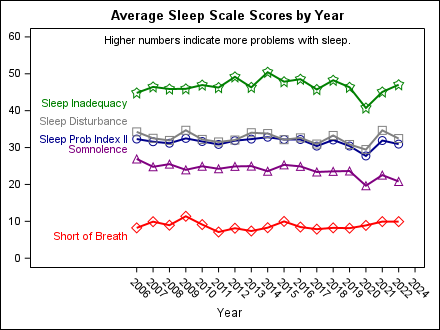
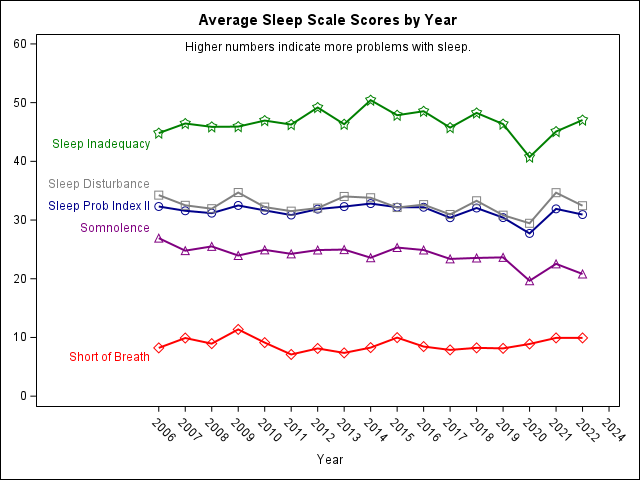
MOS Sleep ScalesThe Medical Outcomes Study (MOS) Sleep Scale is intended to assess the extent of sleep problems. There are several dimensions that make up the scale. The graph above shows the 4 subscales that make up the Sleep Problem Index II – Sleep Inadequacy, Sleep Disturbance, Somnolence, and Short of Breath. All of the scales in the graph range from 0 to 100 with higher numbers indicating more problems with sleep. Several questions about the quality and duration of your sleep over the past 4 weeks are asked. Different calculations are used for each sleep measurement.
Sleep Inadequacy can be defined as a combination of insufficient sleep duration and sleep quality. It can also be described as not getting enough sleep to feel rested upon waking up.
Sleep Disturbance refers to problems initiating or maintaining sleep.
Somnolence means sleepiness or feeling drowsy during the day.
Short of breath, within the MOS Sleep Scale, is determined by the question, “how often during the past 4 weeks did you awaken short of breath or with a headache?”
Sleep Problem Index II is the average of the 4 subscales listed above and gives an overall sleep score ranging from 0 to 100.
Mental Health
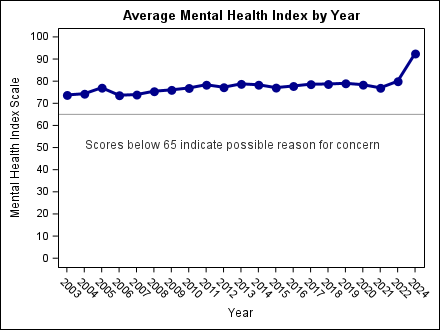
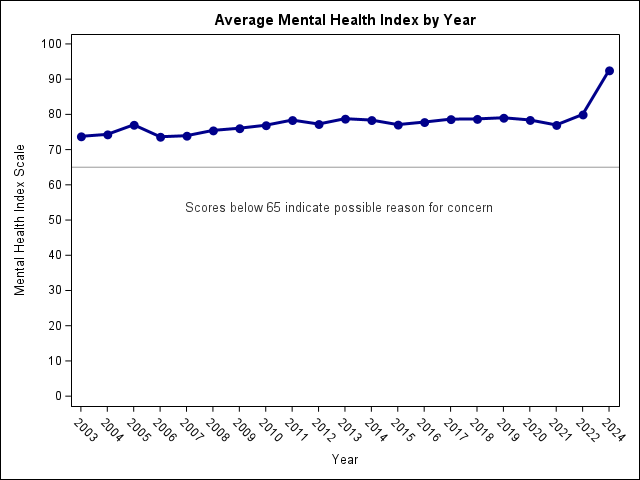
Mental Health Inventory (MHI-5)The five-item Mental Health Inventory (MHI-5) is a very brief questionnaire about your mood used to assess mental health. The score ranges from 0 to 100 with a lower score indicating worse mood.
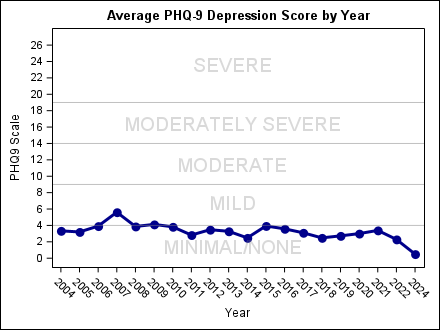
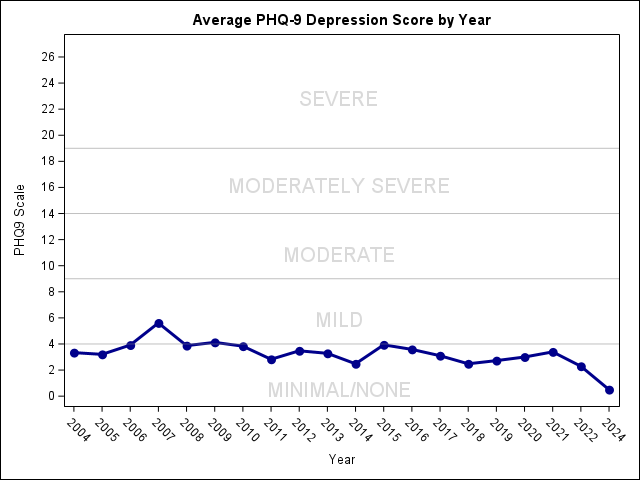
Patient Health Questionnaire (PHQ-9)The Patient Health Questionnaire – depression module is a multipurpose instrument for measuring the severity of depression. It incorporates DSM-IV depression diagnostic criteria with other leading major depressive symptoms into a brief self-report tool.
0 – 4 = none/minimal depression
5 – 9 = mild depression
10 – 14 = moderate depression
15 – 19 = moderately severe depression
20 – 27 = severe depression
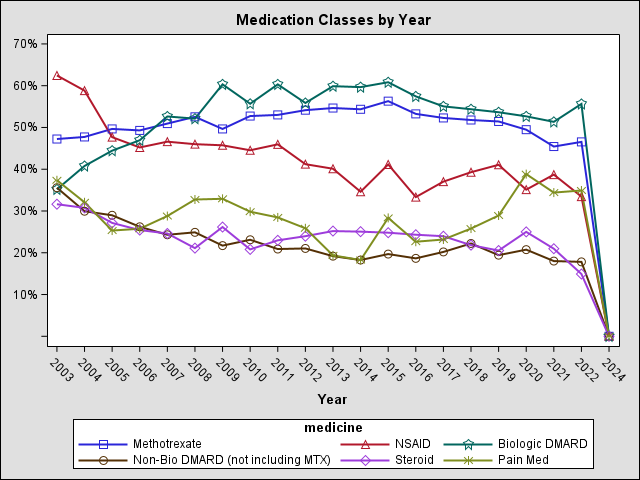
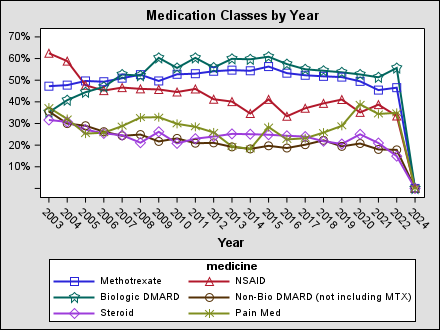
Medications
Medications by Year Biologic DMARDs
Biologic Disease Modifying Anti-Rheumatic Drug
Biologics target specific parts of the immune system to help reduce the inflammation process. These drugs can work quickly to reduce joint pain and swelling. In the longer term, biologics have been shown to slow the pace of joint damage and to improve joint use and movement. The first biologic was approved by the FDA in 1998. Several more biologics have been approved over the years. Common biologics are Enbrel (etanercept), Remicade (infliximab), Humira (adalimumab), Kineret (anakinra), Orencia (abatacept), Rituxan (rituximab), Cimzia (certolizumab), Simponi (golimumab), Actemra (tocilizumab), and Xeljanz (tofacitinib).
Non-Biologic DMARDs
Disease Modifying Anti-Rheumatic Drugs
These drugs can slow or stop progression of joint damage by suprressing the immune system. The most commonly used DMARDs are Plaquenil (hydroxychloroquine), Arava (leflunonomide), methotrexate, and Azulfidine (sulfasalazine).
NSAIDs
Nonsteroidal anti-inflammatory medications, such as celecoxib (Celebrex), ibuprofen, or naproxen reduce inflammation and help relieve pain. NSAIDs do not slow joint damage.
Pain Medications
This group includes narcotics, such as Oxycontin (oxycodone) and Vicodin (hydrocodone), as well as non-narcotic pain relievers such as acetaminophen.
Steroids
Corticosteroids are strong inflammation fighters that can quickly improve symptoms and reduce swelling. They are less effective at slowing the disease itself. They may be prescribed to get inflammation under control, or when you have a flare. For some people, a very low dose of steroids taken by mouth in combination with DMARDs and/or biologics seems to control their RA.
DMARD Usage at Most Recent VisitClick on graph for larger image
The biologics pie chart shows the percent of BRASS patients on each biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of biologic. Patients could also be on another type of medication.
The non-biologics pie chart shows the percent of BRASS patients on each non-biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of non-biologic DMARD. Patients could also be on another type of medication.








 Click on graph for larger image
The biologics pie chart shows the percent of BRASS patients on each biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of biologic. Patients could also be on another type of medication.
The non-biologics pie chart shows the percent of BRASS patients on each non-biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of non-biologic DMARD. Patients could also be on another type of medication.
Click on graph for larger image
The biologics pie chart shows the percent of BRASS patients on each biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of biologic. Patients could also be on another type of medication.
The non-biologics pie chart shows the percent of BRASS patients on each non-biologic medication. It is using patient-reported medication use as of the most recent BRASS visit and only includes those reporting that they were on some sort of non-biologic DMARD. Patients could also be on another type of medication.